
Many military members do not seek mental health services because they don’t think getting that care will remain private — and that concern is not unwarranted, according to a new report.
Fear of their treatment becoming known to coworkers creates “clear disincentives to mental health care for military members,” according to a new report from the RAND Corporation. Confusion over when and how their medical information — including mental health diagnoses — can be handed over to their chain of command is common, with both troops and leaders.
Though there are tight rules that govern that access, many leaders are either unaware or have different interpretations of them, the RAND report found. In one instance, a commander told the report’s authors that he believed all mental health treatments in a military member’s past should be open to commanders, including treatments they may have had before joining, even as children.
The report went on to note that concerns over a lack of confidentiality cause service members to keep mental health issues private, and to defer or avoid care, end treatment, or not report warning signs like workplace errors, violent, or suicidal ideation.
Among troops who consider seeking mental health treatment, RAND found that more than half fear that their records would be shared with promotion review boards, future civilian employers, and future medical insurers.
‘No risk’ for most treatment seekers
A 2022 Military Medicine journal study that analyzed research on Air Force and Marines Corps personnel found those who sought mental health treatment on their own — dubbed “self-referral” — were “less likely to face career-affecting provider recommendations” than those directed to mental health services by their commands, though data on command-directed care, RAND found, is “not consistent.” The researchers hypothesized that those who self-refer get help “before their problems even reach diagnosable levels,” but also said that the data was not sufficient to compare the two groups. They did conclude, however, “for the vast majority of treatment-seekers, there is no risk.”
According to the Pentagon’s annual suicide report released in November, since 2011, active duty suicide rates have steadily increased but less than half of the 363 active-duty troops who committed suicide in 2023 had one or more mental health diagnoses — meaning they met with a provider and were formally diagnosed with a mental health condition. For the National Guard and Reserve, service members with previous diagnoses made up nearly one-third of troops who committed suicide, although that number may be low because the majority of National Guard and Reserve troops don’t access care through the military.
The RAND report suggested that leaders can help mitigate these fears by addressing situations where treatment could lead to career impediments. Commanders, the report said, should make efforts to ensure treatment does not impact a deployment, work to mitigate stigmas and enforce privacy protections with a “need-to-know requirement to include as few individuals as possible.”
In interviews with providers, service members, and commanding officers, the report found different opinions on the “minimum amount of information” that should be shared about a service member’s mental health treatments.
The report found that at least one commanding officer argued that a member’s mental health treatment should be open to full disclosure and should even include information going back to before a service member joined, possibly even to their childhood.
“I personally think that childhood trauma has a lot of impact on how [service members] behave during enlistment. If we did a better job holistically understanding a [service member] and their upbringing and ask questions about family and seeing if there is a past trauma, that often helps explain behaviors,” one commanding officer told RAND. “This is coming from a dude with zero clinical experience, but I have read as many books on the subject.”
Misperceptions among troops about what warranted command notification for mental health treatment were widespread:
- Around 56% thought commands were notified if a service member missed a mental health appointment, which would tip off workplaces that the service member was seeking mental health treatment.
- Nearly 35% thought that if they moved to a new duty station, their new commander would be informed of any mental health diagnosis when they arrived at a new duty station.
- Just under 32% thought notification was required for any mental health-related prescription. Almost 31% thought it applied to any mental health diagnosis.
Even if troops do access care through the military, almost 90% indicated they would limit what they share with mental health providers because of privacy concerns. More than 40% said they would seek treatment in the civilian world or get care after hours.
The report acknowledged that it’s “unclear whether this can ever be fully remedied” but that one solution could be restricting command releasable information “to be solely about duty limitations.”

Command notification
One of the RAND survey’s main findings was a lack of understanding of command notification policies regarding personal health information. According to RAND, “a sizable percentage” of respondents incorrectly thought that notification was required in cases where they were not.
Rules about patient information that a commander can see fall under several layers of authority. The Department of Defense, the Defense Health Agency and individual services each have rules in place on mental health privacy protections and circumstances for disclosure. But according to RAND, “the definitions and guidance provided in the policies still leave room for interpretation and discretionary judgment.”
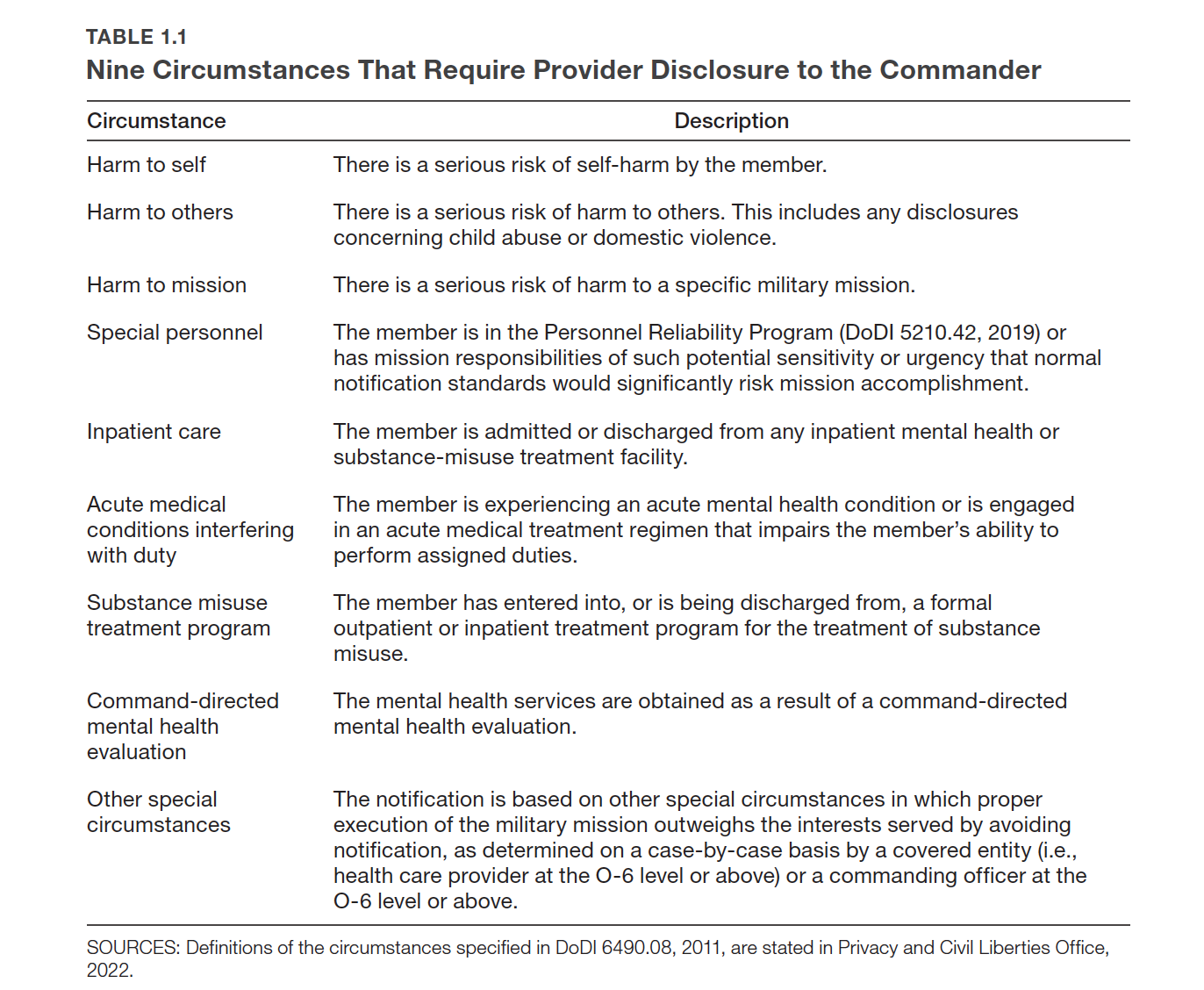
The DOD has nine circumstances under which providers would be required to disclose otherwise protected health information, according to the Defense Department instruction, including potential for self-harm and harm to others, or if the patient works with nuclear weapons.
However, being outside of the clear-cut areas for disclosure might not protect all patients. The report gives the example of a drone operator experiencing anxiety or self-doubt and how that issue could have “the potential to harm a mission.” That information could be released under a DOD policy of “other special circumstances.”
Providers and commanding officers told RAND that suicide and homicide ideation warranted reports to the chain of command as well as mental health concerns that affect the unit’s mission. As for defining what “harm to mission” looks like, the study received varying responses but most agreed that it depended on the job or unit.
The RAND report found a lot of confusion over service members who displayed behaviors that could cause potential harm to themselves or others. One commanding officer said they would tell the command about someone expressing suicidal ideation because of readiness impacts. But a provider said: “I see a lot of folks with morbid ideations, with severe symptoms; that doesn’t necessarily warrant command communication.”
Existing policies that limit privacy
Barriers to accessing mental health resources have resulted in service member suicides like Petty Officer 3rd Class Brandon Caserta who threw himself into a helicopter’s spinning tail rotor in June 2018 after he was bullied by a supervisor and was unable to find mental health resources. After his death, Congress included the Brandon Act, in the fiscal year 2022 defense bill which created a process for service members to seek mental health resources confidentially by asking for an E-5 and above supervisor referral for an evaluation. The policy also requires commanders or supervisors to refer their troops as soon as practical and that service members can use duty time to attend their appointments.
The Defense Department has been working on a phased approach of the measure, beginning with active duty personnel, but the RAND report said “it remains unclear” how the policy preserves privacy or enhances current protections of service member self-referrals to mental health support without command involvement.
The Defense Health Agency did not respond to requests for comment.
RAND officials recommended better training and education on all current policies. Providers told RAND that they sometimes relied on their networks, medical-legal consultants or “word of mouth” for questions about confidentiality. Some commanding officers even turned to Google.
One enlisted service member said they didn’t know how to access regulations that spell out mental health privacy protections, telling RAND: “There’s two trillion of those and they aren’t worded clearly,” they said.
The report also noted a lack of empirical data around the “effectiveness of confidentiality policies” and suggested future research look at how increasing privacy protections could improve mental health resource uptake. They also recommended that the Defense Health Agency expand treatment with more privacy like telehealth and behavioral health resources outside of work hours.